




Criminal justice reform; treatment and functional change; sanctions and incentives
savvy
Bipartisan consensus and collaboration in the current US political environment is almost unheard of. There is, however, one area where many have agreed to take action. From the President on down and across the political aisle, there has been bipartisan agreement to focus on criminal justice reform. The United States:
- Incarcerates more of its population than any other country.
- Has only 5% of the world’s population, but 25% of the world’s prisoners.
- Keeps 1 in 33 Americans under correctional control (1).
Fortunately, there is increasing agreement that the high economic and societal costs of incarceration could be reduced if we focus on treatment for those among the incarcerated population who are suffering from the disease of addiction.
- Individuals with substance use disorder (SUD) represent a significant proportion of those behind bars.
- Half of federal prisoners are incarcerated on drug-related offenses (2).
- 85% of prisoners are there for substance-related reasons. This means they either have an active or prior SUD or committed their crime while intoxicated or to obtain money for drugs (3).
- SUD is also highly prevalent among probationers and two-thirds are alcohol or drug involved (4).
In many cases these offenses are a manifestation of the disease of addiction rather than a criminal proclivity, so providing addiction treatment is effective in preventing legal recidivism.
- Most prisoners do not receive treatment from a trained clinician despite the fact that addiction is a treatable disease (2).
- Research has shown that treatment improves clinical outcomes and reduces crime, recidivism, and societal costs.
- However care within correctional facilities remains heterogeneous; it often does not meet community standards of care.
- The most striking example is the lack of access to pharmacotherapy, despite strong evidence for the efficacy of these treatments (5).
I am a Senior Fellow in the Justice Programs Office (JPO) of the School of Public Affairs (SPA) at American University, Washington, DC. In this capacity, I have had an opportunity to open up an important conversation. In February I presented the first in an interactive webinar series on Critical Treatment Issues: “What to expect from state-of-the-art addiction treatment for criminal justice populations in applying the new American Society of Addiction Medicine (ASAM) Criteria.” This is a part of the Bureau of Justice Assistance (BJA), US Department of Justice, Drug Court Technical Assistance Project at American University.
* If you’d like to review the recorded sessions and/or register for upcoming webinars, read SHARING SOLUTIONS below.
TIP 1
Addiction treatment is assessment and outcomes-driven, not program and compliance-focused.
Note these definitions of Compliance and Adherence -Webster’s Dictionary defines “comply” as follows: to act in accordance with another’s wishes, or with rules and regulations.
It defines “adhere“: to cling, cleave (to be steadfast, hold fast), stick fast.
The criminal justice system correctly focuses on Compliance, Consequences and Control. If laws of the land are to Control public safety, then everyone has to Comply. If people do not Comply, there have to be Consequences.
Look back at the November, 2007 edition of Tips & Topics. There I wrote more on the contrast between the mission of criminal justice versus the focus of addiction treatment.
- Judges and court teams increasingly realize it is worth offering treatment to offenders whose drug-related criminal record is related to their addiction illness, not just criminal behavior.
- Offering treatment to such an offender improves the chance for increased public safety and decreased legal recidivism and crime.
- When the court team is gracious enough to offer treatment as an alternative to incarceration, treatment providers must ensure assessment and outcomes-driven services which help participants make actual changes that increase public safety.
- That requires the focus to be on individualized treatment, not on compliance (acting in accordance with others’ wishes and rules and regulations) in a program.
- Individualized treatment starts with participant multidimensional assessment, which identifies Problems and Priorities arising from each person’s Severity of Illness (SI) and Level of Function (LOF). The collaborative Treatment Plan defines the Intensity of Services needed; and that should encompass a wide variety of evidence-based Modalities delivered in a Levels of Service continuum.
- How a participant Progresses through treatment depends on improvement in SI and LOF. If the participant is improving such that public safety is increased, then the treatment provider assesses what needs to be done next. If the participant is not progressing in function well, the treatment provider assesses what the problem is and how to change the treatment plan.
This is the cycle of Individualized, assessment and outcomes-driven services:
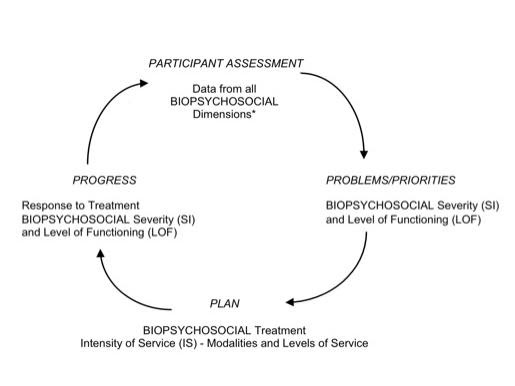
* ASAM Criteria Multidimensional Assessment
- Acute Intoxication and/or Withdrawal Potential
- Biomedical conditions and complications
- Emotional/Behavioral/Cognitive conditions and complications
- Readiness to change
- Relapse/Continued Use/Continued Problem potential
- Recovery Environment
TIP 2
Structure the phases in drug and other specialty courts based on functional milestones, not on time and compliance.
Usually the “phases” are structured in terms of time frames and tasks rather than achievement of functional milestones. Such phases, without functional milestones, too easily promote compliance ,”Doing Time” vs. adherence “Doing Treatment and Change.”
Compare and contrast these sets of Phase language:
A. Compliance style phase language
Orientation Phase, Length of Phase – Minimum of two (2) months.
A. Functional change style phase language
Orientation Phase, Length of Phase – Minimum of two (2) months; or earlier, in collaboration with treatment provider, if functional change achieved.
B. Compliance style phase language
Attendance at NA/AA meetings (if required to attend by the court). Identify a home group, attend frequently, and begin to identify with a sponsor.
B. Functional change style phase language
Identification of support group; attend 12-Step or other support group in collaboration with treatment provider who assesses what is the most effective support group as part of the individualized treatment plan (Assess participant’s Dimension 6, Recovery Environment).
C. Compliance style phase language
Advancement to next phase – Participant must be compliant with all court appearances and treatment recommendations, be actively participating in substance abuse treatment, participating in 12 step Fellowship meetings (if required to attend), complying with ancillary services if referred or recommended by Court and/or treatment provider), have completed any sanctions imposed and provided negative urinalysis for minimum of two consecutive months.
C. Functional change style phase language
Advancement to next phase – Consistent attendance, demonstrating functional improvement in problems that threaten public safety or increase legal recidivism and crime. (Review all six ASAM Criteria dimensions e.g, Dimension 2, chronic pain; Dimension 3 co-occurring disorders or impulsivity; Dimension 4 stage of change; Dimension 5 coping skills to not use; Dimension 6 friends, family, work, finances etc.)
References
1. Pew Center on the States (2008). One in 100: behind bars in America 2008. (http://www.pewcenteronthestates.org/uploadedFiles/8015PCTS_Prison08_FINAL_2-1-1_FORWEB.pdf.) 2. Mumola CJ & Karberg JC. Drug Use and Dependence, State and Federal Prisoners, 2004. Bureau of Justice Statistics, October 2006, NCJ 213530. 3. CASA Columbia, 2010. Behind Bars II. http://www.casacolumbia.org/addiction-research/reports/substance-abuse-prison-system-2010. 4. Mumola CJ. Substance Abuse and Treatment of Adults on Probation, 1995. Bureau of Justice Statistics. March 1998, NCJ 166611. 5. Bruce RD, Smith-Rohrburg D, Altice FL. (2007) Pharmacological treatment of substance abuse in correctional facilities; prospects and barriers to expanding access to evidence-based therapy. In R Greifenger (Ed) Public Health Behind Bars; from prisons to communities. (pp 385-411) Springer.
skills
It is challenging to make the shift from compliance-driven programs to individualized, outcomes-driven services. Such a change holds everyone accountable for achieving real functional change- both the participant and the treatment provider. It requires collaboration between the court team and the treatment provider.
TIP 1
Give the judge and the court team robust information. Report on whether the participant is improving in function that increases public safety.
Many treatment providers report just on the participant’s compliance with court orders:
1. Attend and participate in treatment and 12-Step support groups.
2. Provide negative drug screens.
3. Abstain from using substances and avoid negative peer influences.
In such reports the attention is all on compliance to court orders. Instead, the focus should be on the more critical level of improvement in function which truly affects the goal of lasting change.
Here are some elements of a robust report to the court:
- The client’s attendance: Is he/she simply attending treatment sessions, without actively adhering to his/her individualized treatment plan?Evidence of adherence: Client knows and follows through on treatment plan strategies designed to increase pro-social attitudes and behavior.
- What if your client is attending but passive in groups and treatment planning – just “doing time” not “doing treatment and change?” In that situation the treatment provider should report that to the court team. The provider might even recommend a graduated sanction since the client is out of compliance with the court order for assessment and treatment adherence.
- Is the client actually changing in attitude, thinking, and behavior in ways that increases public safety and decreased likelihood of re-offending?
What does the evidence look like? A client is changing attitudes and behavior such as staying away from “toxic” friends and family. Or, the client is relating differently to co-occurring physical or mental health challenges that threaten their sobriety e.g., chronic pain or trauma. Or they are demonstrating coping strategies to deal with cravings and temptations to use alcohol or other drugs. - What if the client is not demonstrating progress and improved function to increase public safety? In that situation the treatment provider collaborates with the client to reassess why progress is not being made. (Review all six ASAM Criteria dimensions to see what has been missed or what has changed.) If it is not clear why outcomes are faltering, consultation should be sought and the court team informed.
- Building social networks to support recovery: Is he/she developing pro-social peer and leisure activities; meaningful work and self-sufficiency in finances and housing?
Here’s what evidence looks like: They are active in AA or NA or other 12-Step recovery groups; or alternately actively involved with SMART recovery groups; or active in a community of faith e.g., church, synagogue or mosque. - If outcomes and progress have stalled, is the client actively participating in changing the treatment plan in a positive direction? Some poor outcomes might be a flare-up of addiction with actual substance use and a positive drug screen; or the client has drifted back to old drug using friends; or diminishing and superficial attendance at self/mutual help groups. Evidence of positive changes in the treatment plan: Client is committed to staying away from drug using neighborhoods; or now sees hanging out with Joey is a major temptation even if he/she is not ready to give up all his other drug-using friends yet. Or client is willing to increase support group meetings by one a week or even everyday that week. (Progress, not perfection in treatment planning.)
- What if the client is not in good faith collaborating on changing the treatment plan in a positive direction? In that situation the treatment provider should alert the court team of the lack of progress in positive functional change. If public safety is increasingly threatened by lack of progress, it is the treatment provider’s duty to report that to the court.
TIP 2
Rethink sanctions and incentives to focus on engagement, improved function and recovery.
1. Sanction for lack of good faith adherence to treatment, not for signs and symptoms of the disease of addiction:
- Many judges mandate abstinence and then sanction for substance use and positive drug screens. Such mandates forget that addiction is a disease characterized by loss of control. If a participant in early treatment can consistently and perfectly control substance use, they are unlikely to have the disease of addiction. Or it may be that they are able to maintain abstinence only when being closely watched and monitored in a controlled environment.
- A major purpose of treatment is to promote lasting self-change. It is important that the participant learns how to self-monitor and resist triggers and temptations to drink or drug. These skills do not happen overnight or just because they are mandated to be abstinent. Most participants may not be perfectly consistent in early stages of treatment and may even use. So long as the client continues to make positive changes, while not being in perfect control, treatment should continue without sanctions for substance use.
- Mental health courts do not mandate non-psychosis, non-anxiety or panic, non-depression or suicidality and then sanction for flare-ups hallucinations, panic attacks or suicide attempts. It is the same for addiction treatment.
- If judges mandate assessment and treatment adherence, then the focus is not on compliance with abstinence, but on adherence to individualized treatment and functional lasting, self-change.
- Graduated sanctions are appropriate for clients who are not collaborating in treatment in good faith. This investment in treatment towards positive change is the treatment provider’s responsibility to monitor and report on to the court team.
2. Create incentives that are person-centered and assessment-based, not generic rewards.
- Generic incentives are like gift certificates and material goods. Instead, collaborate with the client to identify meaningful incentives that promote recovery.
- For example: if a participant has been restricted from seeing his/her children and wants to restore that trust, working on sobriety and recovery will help meet that goal. It would be a meaningful incentive for us to advocate with the family or child protective services for supervised visits, so long as the client was working in treatment in good faith.
- Or perhaps a client wants a better living situation or job. Helping them to explore different apartments or arrange informational interviews with potential employers can be meaningful incentives.
In the September 2014 edition of Tips & Topics, I suggested some perspectives on sanctions and incentives.
soul
This Easter while we were away for the weekend, a would-be robber threw a brick through the window next to the front door. They reached in and unlocked the door ready to steal anything that could be turned into quick cash. Things to be grateful for:
- No one was home, so no one was hurt.
- Our home security alarm shrieked on cue and scared the would-be robbers away.
- Nothing was stolen, even though they did leave a “gift” of a bucketful of shattered glass.
- It could have been much worse had they had gotten frustrated and trashed the house.
- Imagine what it would be like to endure physical and emotional violence in rape, physical and sexual abuse, assault and real trauma? This is just a tiny fleabite in comparison.
- Our trusted handyman interrupted his Easter Sunday religious and family activities to board up the window and secure the house.
- Our faithful neighbor checked out the house and gave up her relaxing Sunday morning to supervise the police visit and securing of the house.
- Southwest Airlines changed my airline ticket to get me home a day earlier with no $200 change fee (not like all those other airlines that milk you for fees at every turn.)
- Even the Airport shuttle had a space open to whisk me home quickly. I was the first passenger dropped-off, so no waiting or circuitous route home. It was almost like my own personal limousine.
We read statistics about home invasions and crime, and it is all so theoretical and such a pity for those “other” people whose homes were robbed. It is all SO different when it becomes personal.
When you do a clinical assessment with a client, and note down his or her arrest record and previous crimes, it is so matter-of-fact and routine. But that client was like my would-be robber who threw the brick through my window invading our space and property.
Of course we’ll never know who it was. What urgent need compelled him/her to commit such a crime? How illuminating it would be to actually talk to and assess that person. What would I say? How would I feel? How would I negotiate restorative justice with this person? (Google “restorative justice” if that system is new to you.)
How was your Easter weekend?
sharing solutions
Past webinars to view
1. “What to expect from state-of-the-art addiction treatment for criminal justice populations in applying the new ASAM Criteria”
– This webinar reviews how addiction is a brain disease with biopsychosocial-spiritual manifestations, causes and treatment needs; and how the ASAM (American Society of Addiction Medicine) criteria is applied to criminal justice clients. It explains what to expect from treatment providers: a comprehensive multidimensional assessment; person-centered, outcomes-driven services and treatment planning. There is discussion about communication issues between treatment providers and court personnel; what to expect of court personnel and the treatment provider.
The recordings can be accessed from the Justice Programs Office’s YouTube page:
Session 1: https://www.youtube.com/watch?v=AuUEP52z1Xk
Follow-up Q&A: https://www.youtube.com/watch?v=rj6FabxX5lk
They are also available on the American University website at: http://www.american.edu/spa/jpo/videos/webinars.cfm
2. “Doing Time or Doing Treatment: Moving beyond Program Phases to Real Lasting Change”
– This webinar addresses the differences in the culture and mission between criminal justice and treatment of addiction. It emphasizes the path to achieving outcomes of increased public safety, decreased legal recidivism and crime, safety for children and families by expecting accountable, real change to reach public safety goals. It contrasts passive, compliant participation in treatment programs phases where clients too often just “do time” in treatment; and discusses the use of incentives and sanctions that promote treatment engagement and sustainable change. There is also discussion about punishing for rule breaking and positive drug tests; and abstinence-oriented versus abstinence-mandated approaches.
The recordings can be accessed from the Justice Programs Office’s YouTube page:
Session 2: https://www.youtube.com/watch?v=KtLi1IPtv6k
Follow-up Q&A: https://www.youtube.com/watch?v=fPWSdoN7wR8
They are also available on the American University website at: http://www.american.edu/spa/jpo/videos/webinars.cfm
Upcoming webinars April 4 and 5, 2016
1. Upcoming session in the webinar series on Critical Treatment Issues:Monday, April 4, 2016 from 1:00 to 2:00 p.m. EDT, with a follow-up interactive web meeting on Tuesday, April 5 from 1:00 to 2:00 pm EDT to address questions participants have that could not be answered during the session.
“Engaging Participants in a Self-Change Process” – Stages of change and “discovery, dropout prevention” plans versus “recovery, relapse prevention” plans; holding participants accountable to an individualized treatment plan based on stage of change versus compliance with program phases and rules; evidence-based practices EBPs), therapeutic alliance and examples of EBPs that engage participants in a self-change process e.g., Motivational Interviewing, CBT, stages of change work, Interactive Journaling.————————————————————————————————————————
To register for the webinar(s):————————————————————————————————————————
1. Go to: https://bja-au.webex.com/bja-au/onstage/g.php?PRID=a6642d1af8e20bd689ac7433ee634daf
2. Choose the webinar event(s) you would like to register for and click Register.
3. On the registration form, enter your information and then click Submit.
4. This will generate an automatic email confirming your registration and providing you with the information to attend the event (the email will be from “messenger”).——————————————————-
Please contact Monica Fuhrmann (fuhrmann@american.edu) if you have any questions on the webinar or the registration process.